Revolutionary therapy slows tumor growth in advanced breast cancer
A novel therapy designed to attack tumors in patients with a genetic mutation in either BRCA1 or BRCA2, slowed tumor growth in 85 percent of advanced breast cancer patients treated in a small study, researchers report in the July 6 issue of the Lancet.
“That is really an enormous response rate in a population of patients who have received a median of three prior therapies,” says study co-author Susan M. Domchek, MD, associate professor of Medicine, University of Pennsylvania School of Medicine, and director of the Cancer Risk Evaluation Program at Penn's Abramson Cancer Center.
“This is the first time that we have been able to take the genetic reason a person has developed cancer and make it a target,” Domchek says. “Most of the time we look at what is going on in the tumor itself and then figure out how to target it. But in this situation, the women all had an inherited mutation in either the BRCA1 or BRCA2 gene and we could exploit that weakness in the tumor. It is a strategy that may cause fewer side effects for patients.”
The new agent, called olaparib, inhibits a protein called poly(ADP-ribose) polymerase (PARP). Both PARP and the BRCA proteins are involved in DNA repair. And while cells seem to be able to do without one or the other, inhibiting PARP in a tumor that lacks a BRCA gene is too much for the cells, and causes them to die.
“If you put too much stress on the cancer cell, it can't take it and it falls apart,” Domchek says. Because the non-tumor cells in a patient with an inherited BRCA mutation still retain one normal copy of the BRCA gene, they are relatively unaffected by PARP inhibition. “These drugs may be very potent in tumor cells and much less toxic in normal cells. That is important from the perspective of cancer treatment,” Domchek says.
The international study enrolled 54 patients in two groups. The first group of 27 women received 400 mg oral olaparib twice daily and the second group of 27 patients received 100 mg oral olaparib twice daily. The higher dose appeared to have more activity against the disease, with one patient (4%) having a complete resolution of her tumor and ten (37%) showing substantial tumor shrinkage. Another 12 (44%) women had stable disease or some tumor shrinkage, but not enough to be considered a partial response by standard criteria. In the low dose group, six (22%) patients showed substantial shrinkage and 12 (44%) had some tumor shrinkage or stable disease.
Although the results look good thus far, Domchek says more clinical trials will be necessary before olaparib or other PARP inhibitors in development will be ready for use in regular practice. “It is important for patients to join those clinical trials because we need to determine how best to use these drugs, on their own or in combination with other agents,” she said. “And we need to establish definitively that they are better than other drugs.”
The PARP inhibitors are a transition in the field of cancer drug development. “This is a different way of looking at cancer therapeutics,” Domchek says. “In oncology, this is really one of the first times that we've seen drugs being developed on the basis of inherited susceptibility – and that may open up a whole new avenue of drug development.”
Penn was one of just six centers in the United States to participate in the clinical trial. The trial was led by Andrew Tutt, MD, of the Breakthrough Breast Cancer Research Unit at Kings College London School of Medicine. Breakthrough Breast Cancer is a pioneering charity dedicated to the prevention, treatment and ultimate eradication of breast cancer through research, campaigning and education. Co-authors on the study are Mark Robson (Memorial Sloan-Kettering Cancer Center, New York), Judy E Garber (Dana-Farber Cancer Institute, Boston), M William Audeh (Samuel Oschin Cancer Institute, Los Angeles), Jeffrey N Weitzel (City of Hope Comprehensive Cancer Center, Duarte, CA), Michael Friedlander (Prince of Wales Cancer Centre, Sydney, Australia), Banu Arun (MD Anderson Cancer Center, Houston), Niklas Loman (Skane University Hospital and Lund University Hospital, Sweden), Rita K Schmutzler (University Hospital Cologne, Germany), Andrew Wardley (The Christie Hospital NHS Foundation Trust, Manchester, UK), Gillian Mitchell (Peter MacCallum Cancer Centre, East Melbourne, Australia), Helena Earl (University of Cambridge and NIHR Cambridge Biomedical Research Centre, UK), and Mark Wickens and James Carmichael (AstraZeneca, Macclesfield, UK).
AstraZeneca provided funding for the trial. Dr. Domchek has no ties to AstraZeneca and no other disclosures to report.
Penn Medicine is one of the world's leading academic medical centers, dedicated to the related missions of medical education, biomedical research, and excellence in patient care. Penn Medicine consists of the University of Pennsylvania School of Medicine (founded in 1765 as the nation's first medical school) and the University of Pennsylvania Health System, which together form a $3.6 billion enterprise.
Penn's School of Medicine is currently ranked #3 in U.S. News & World Report's survey of research-oriented medical schools, and is consistently among the nation's top recipients of funding from the National Institutes of Health, with $367.2 million awarded in the 2008 fiscal year.
Penn Medicine's patient care facilities include:
The Hospital of the University of Pennsylvania – the nation's first teaching hospital, recognized as one of the nation's top 10 hospitals by U.S. News & World Report.
Penn Presbyterian Medical Center – named one of the top 100 hospitals for cardiovascular care by Thomson Reuters for six years.
Pennsylvania Hospital – the nation's first hospital, founded in 1751, nationally recognized for excellence in orthopaedics, obstetrics & gynecology, and behavioral health.
Additional patient care facilities and services include Penn Medicine at Rittenhouse, a Philadelphia campus offering inpatient rehabilitation and outpatient care in many specialties; as well as a primary care provider network; a faculty practice plan; home care and hospice services; and several multispecialty outpatient facilities across the Philadelphia region.
Penn Medicine is committed to improving lives and health through a variety of community-based programs and activities. In fiscal year 2008, Penn Medicine provided $282 million to benefit our community.
Media Contact
More Information:
http://www.uphs.upenn.eduAll latest news from the category: Health and Medicine
This subject area encompasses research and studies in the field of human medicine.
Among the wide-ranging list of topics covered here are anesthesiology, anatomy, surgery, human genetics, hygiene and environmental medicine, internal medicine, neurology, pharmacology, physiology, urology and dental medicine.




Newest articles
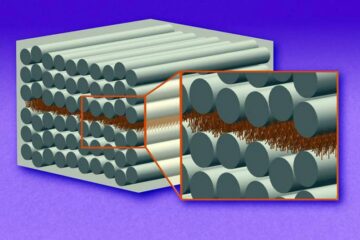
“Nanostitches” enable lighter and tougher composite materials
In research that may lead to next-generation airplanes and spacecraft, MIT engineers used carbon nanotubes to prevent cracking in multilayered composites. To save on fuel and reduce aircraft emissions, engineers…

Trash to treasure
Researchers turn metal waste into catalyst for hydrogen. Scientists have found a way to transform metal waste into a highly efficient catalyst to make hydrogen from water, a discovery that…
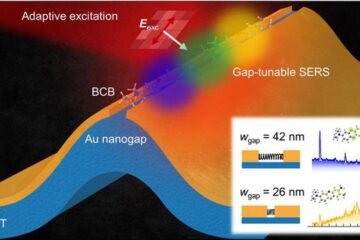
Real-time detection of infectious disease viruses
… by searching for molecular fingerprinting. A research team consisting of Professor Kyoung-Duck Park and Taeyoung Moon and Huitae Joo, PhD candidates, from the Department of Physics at Pohang University…

