When a reaction to adverse life events becomes a mental disorder
According to the Author, this problem is becoming so visible only now because of different factors: 1)the recent broadening of the scope of psychiatric intervention from traditional hospital settings, where the issue whether admitted patients had or did not have a mental disorder was not really relevant, to community settings, where this issue is a sensitive one in several cases;2)the increased presence and influence in the mental health field of several other professions, whose perception of mental health problems is often different from that of psychiatrists; 3)the higher level of information and awareness of users, families and the public opinion.
Even if now psychiatrists have specific diagnostic criteria, the threshold for the diagnosis of some mental disorders appears more clearly arbitrary today than in the past. Three possible approaches for addressing this issue are proposed by Prof May.
The first approach is the one emphasizing the context in which the symptoms occur (i.e., the diagnosis of depression should be excluded if the sadness response is caused by a real loss that is proportional in magnitude to the intensity and duration of the response).
A second approach to the problem is the one emphasizing possible ‘qualitative’ differences between true mental disorders and homeostatic reactions to adverse
events and some recent studies have revived the research line exploring the nature of the ‘distinct quality of mood’ which differentiates at least some forms of depression from understandable sadness.
The third approach to the problem is the one assuming that the boundary between some mental disorders and homeostatic reactions to adverse events is unavoidably
arbitrary and has to be decided on pragmatic grounds (i.e., the respondent’s
symptoms led him or her to mention them to a doctor or other professional, or the symptoms interfered with his or her everyday life, or the respondent took medication for the symptoms). This criterion, however, does not really discriminate between true mental disorders and transient homeostatic reactions, because the latter can interfere significantly with everyday life.So, it is clear that the issue of the differential diagnosis between some mental disorders (in particular mood and anxiety disorders) and homeostatic reactions to life events is at present completely open. Further research is absolutely needed.
Media Contact
More Information:
http://www.karger.comAll latest news from the category: Health and Medicine
This subject area encompasses research and studies in the field of human medicine.
Among the wide-ranging list of topics covered here are anesthesiology, anatomy, surgery, human genetics, hygiene and environmental medicine, internal medicine, neurology, pharmacology, physiology, urology and dental medicine.




Newest articles
High-energy-density aqueous battery based on halogen multi-electron transfer
Traditional non-aqueous lithium-ion batteries have a high energy density, but their safety is compromised due to the flammable organic electrolytes they utilize. Aqueous batteries use water as the solvent for…

First-ever combined heart pump and pig kidney transplant
…gives new hope to patient with terminal illness. Surgeons at NYU Langone Health performed the first-ever combined mechanical heart pump and gene-edited pig kidney transplant surgery in a 54-year-old woman…
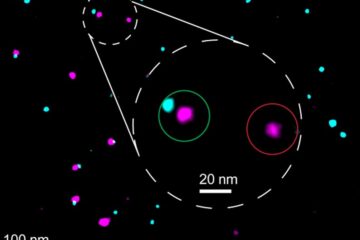
Biophysics: Testing how well biomarkers work
LMU researchers have developed a method to determine how reliably target proteins can be labeled using super-resolution fluorescence microscopy. Modern microscopy techniques make it possible to examine the inner workings…

