Efforts to improve hospital care
In recent years, American hospitals have made significant improvements on standardized, evidence-based measures of clinical performance for several medical conditions, including heart attacks, heart failure, and pneumonia. But an editorial, published in the July 21 issue of the New England Journal of Medicine, says it’s not clear how much effect these improvements in patient care have had on public health, especially in reducing morbidity and mortality. The editorial, authored by Patrick S. Romano, professor of general medicine at UC Davis School of Medicine and Medical Center, is published along with two new quality-of-care studies.
“Evaluating how hospitals deliver medical care does standardize practices and improve care,” says Romano. “For example, hospitals are now more likely to give aspirin and beta blockers to heart attack patients, to evaluate heart failure patients appropriately, to provide complete instructions when patients go home, and to counsel smokers to quit. But we do not yet have evidence that these improvements are reducing morbidity and mortality from heart disease, heart failure and pneumonia.”
In the editorial, Romano analyzes two studies that used standardized, evidence-based measure to evaluate and improve hospitals’ quality of care. One study, from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), describes results from a program in which hospitals seeking accreditation were required to collect and submit data on clinical performance on 18 measures for acute myocardial infarction, heart failure and pneumonia. The other, from the Centers for Medicare and Medicaid Services (CMS), reports on several of the same measures as the JCAHO study.
“These studies didn’t find any reduction in early deaths from heart attacks, deaths among newborns, or injuries during delivery,” said Romano. “Perhaps the benefits of improving care in hospitals aren’t visible until several months or years after hospitalization. Or perhaps some hospitals have figured out how to make their performance look better, without actually improving care at the bedside. Or perhaps other aspects of care, which we aren’t currently measuring, have not improved over time.”
In the JCAHO study, the continuously participating hospitals improved significantly on 15 of the 18 measures for the targeted conditions. The improvement occurred “on every measure that involved appropriate use of medications or provision of counseling, and the trend was favorable for all three of the measures that did not show statistically significant improvement.” Hospitals with the poorest initial performances improved the most over the two-year period studied by the JCAHO team.
The CMS study reports on the variations in clinical performance during the first half of 2004 among hospitals participating in the CMS Hospital Quality Alliance Program. The CMS study reports on several of the same measures as the JCAHO study, and its findings complement those of the JCAHO research, Romano states.
In discussing the implications of the two studies for the future of improvements in quality in the U.S. hospital industry, Romano states, “They establish that very high levels of adherence with evidence-based guidelines are achievable, with sufficient education of physicians and hospital managers and sufficient attention from outside entities such as JCAHO and CMS.” However, Romano adds that “these high levels of adherence may be somewhat illusory, since physicians and hospitals have become increasingly clever at documenting questionable contraindications to standard therapies, thereby excluding many patients who might have benefited from them.”
The studies also confirm that variation in hospital performance, at least for the three medical conditions monitored, has generally diminished in recent years. In addition, the studies confirm “the long-recognized fact that repeatedly observed behaviors improve over time.”
However, Romano questions how broadly the results of the studies can be extrapolated to draw conclusions about improvements in the quality of hospital care generally, or even about care for the specific conditions studied. He notes that the JCAHO and CMS investigators chose to focus on acute myocardial infarction, congestive heart failure and pneumonia because they frequently lead to hospitalization and death, and because medical therapy for these conditions is clearly effective.
“However,” Romano writes, “these conditions do not account for the majority of hospitalizations in the United States. We have no idea whether care for other conditions has deteriorated, even while care for acute myocardial infarction, congestive heart failure and pneumonia has improved. It is even possible that unmeasured aspects of care for these three conditions has deteriorated.”
Romano points out that the JCAHO study did not find any decrease in inpatient mortality for heart attacks, neonatal mortality or obstetric lacerations, which suggests “that the effect of the reported improvements on public health may be modest.”
Despite the gains made in hospital care for the three medical conditions that were the focus of the JCAHO and CMS studies, Romano states that the hospitals “still face major challenges.” Because medical knowledge continues to expand, “practice guidelines and the measures of quality on which they are based require continual updating.”
Romano also states that because hospitals and physicians are becoming “more sophisticated in ’gaming’ quality measures, sponsors must also become more sophisticated in monitoring accuracy.
“For example,” Romano states, “the largest absolute improvements between 2002 and 2004 were documented for smoking-cessation counseling and discharge instructions, which are measures that hospitals can manipulate through check-off forms that nurses complete when they discharge patients with the target conditions. Educational interventions that are effective in a clinical trial may fail abysmally when they are transformed into a check box on a discharge form.”
Despite the improvement documented in the JCAHO and CMS studies, Romano states, “we must not rest on our laurels and assume that we have solved the problem of quality.”
Romano writes, “We have barely begun to touch quality-related problems in mental health and substance-abuse care, pediatric care and home health care. As physicians and health professionals, we have made a little progress, but we still have far to go.”
Media Contact
More Information:
http://www.ucdmc.ucdavis.eduAll latest news from the category: Health and Medicine
This subject area encompasses research and studies in the field of human medicine.
Among the wide-ranging list of topics covered here are anesthesiology, anatomy, surgery, human genetics, hygiene and environmental medicine, internal medicine, neurology, pharmacology, physiology, urology and dental medicine.




Newest articles
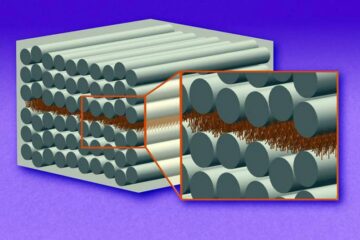
“Nanostitches” enable lighter and tougher composite materials
In research that may lead to next-generation airplanes and spacecraft, MIT engineers used carbon nanotubes to prevent cracking in multilayered composites. To save on fuel and reduce aircraft emissions, engineers…

Trash to treasure
Researchers turn metal waste into catalyst for hydrogen. Scientists have found a way to transform metal waste into a highly efficient catalyst to make hydrogen from water, a discovery that…
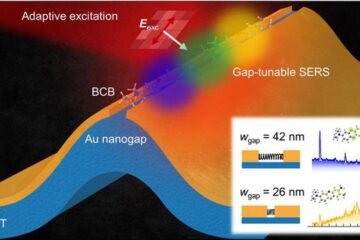
Real-time detection of infectious disease viruses
… by searching for molecular fingerprinting. A research team consisting of Professor Kyoung-Duck Park and Taeyoung Moon and Huitae Joo, PhD candidates, from the Department of Physics at Pohang University…

